In June 2021 Manuela Perrotta and I responded to the government’s call for evidence to inform their forthcoming Women’s Health Strategy for England. The government consultation received over 110,000 public survey responses and over 400 written responses. Just before the December holidays, the Department of Health & Social Care published their vision for the Strategy based on the responses received. Reflecting the sentiments shared in the public survey, the department’s vision highlights fertility, pregnancy, pregnancy loss and postnatal support as particular areas of concern. This grouping of priority areas was the second most selected option across all survey participants (after menstrual health and gynaecological conditions), and the most selected priority area for those aged 30 to 39. Infertility and fertility treatment are integral parts of this broader concern with reproductive and maternal health.
The vision document highlights the need for ‘more trusted and easier to understand information’ about women’s health issues, including reproductive health, which is a key point that we address in our written evidence. In our submission we emphasised that there is an abundance of information about infertility and fertility treatments, especially online. But prospective and current fertility patients often find the information difficult to navigate and identifying good quality information can be challenging. We found that our study participants generally felt that NHS websites offered good sources of reliable information. In our written evidence, we suggest ways for NHS websites to expand their remit to cater for fertility patients’ needs. We were excited therefore, to learn that one of the next steps for the Strategy will be to progress the quality of online information in collaboration with NHS Digital. We hope that the needs of fertility patients will be addressed in this continued work. We also look forward to following further developments as well as the government’s dedicated Sexual and Reproductive Health Strategy, which is expected later this year.
At the beginning of December, we kept up our tradition of attending the Progress Educational Trust’s (PET) annual conference. The title and topic of this year’s online event was ‘Reproducing Regulation: Who Regulates Fertility and How?’ With 16 talks across the full day, I have chosen just a handful here that I thought were particularly pertinent to the issues that we consider in our research.
The first speaker of the day was Julia Chain, chair of the Human and Embryology Authority, who had made headlines in the run-up to the conference with her call for changes to the 1990 Human Fertility and Embryology Act. Her proposed changes would enable the HFEA to impose economic sanctions on fertility clinics that mis-sell unproven treatment add-ons. While she emphasised that her call was not a complete rejection of the current regulatory framework, she highlighted the need to update certain areas of the act to reflect the current state of society and the fertility sector. Currently, she noted, the HFEA has no powers to regulate the increasingly commercialised provision of services. Private fertility treatment is increasingly the norm in the UK, with 65% of IVF treatment being self-funded by patients themselves.
Reflecting on the commercialised fertility sector, Raj Mathur from the British Fertility Society brought attention to questions of fairness and equity and the lack of NHS funding for fertility treatment. Many prospective patients, he reminded us, do not have any access to IVF and when they do, affordability is a huge cause of concern. Mathur spoke about the challenges for patients who have to navigate very complex regulations around the provision of funding, before they even reach the point of having to choose between different treatment offerings.
A significant challenge to regulating the fertility sector is the fast pace of innovation. In her talk entitled ‘What is an add-on, and who gets to decide?’ Anja Bisgaard Pinborg, a specialist in reproductive medicine at Copenhagen University, detailed the difficulties of regulating add-ons safely without stifling the progress of medical research. She explained how the European Society of Human Reproduction and Embryology (ESHRE) is working on a new guideline for regulating add-ons. This guideline includes a very extensive range of tests, treatments and techniques, which reflects the vast and complex offerings of the fertility sector. While Bisgaard Pinborg recognised the obligation of clinics to offer the best treatment to their patients and the strong desires that patients may have to try certain (perhaps more experimental) treatments, she also highlighted that patients should never bear the cost of innovation. Patients, she argued, should not pay for add-ons that are still under development. How fertility patients and professionals navigate the complex world of IVF add-ons is something we have covered extensively in our research publications, workshops and in this blog post on how to best support patients’ informed decisions.
Further examples of how the law and regulation lag behind change were raised by Emily Jackson later in the day. Jackson set out how definitions of ‘mother’ in UK fertility law do not easily apply to the new social and family formations that are enabled though reproductive technologies. Currently, the legal definition of mother is defined in terms of who physically gives birth to a child. One of the examples presented by Jackson involved the case of a child that has two female parents at birth. In this case, the person who gives birth is the mother and the partner is the second legal parent. This is also the case when the partner’s egg was used in the IVF treatment. Interestingly in this case, as Jackson pointed out, the second parent is actually the child’s closer genetic relation. Fatherhood on the other hand, is expressed in both genetic and social terms, which allows for greater flexibility and choice in how fatherhood is defined.
Again, this year’s PET conference succeeded in traversing a wide range of perspectives on the most pressing issues confronting the fertility sector right now.
We are so glad to have hosted two more workshops on The IVF Experience with such kind and active participants! Natalie Silverman, from The Fertility Podcast, enthusiastically commented on the research findings we were introducing in dialogue with many others in our virtual room. We reflected upon how control can be difficult in the IVF journey, and about the benefits or challenges of sharing one’s experience with other patients during treatment. Some of our participants exchanged ideas about the resources available to fertility patients or donors when it comes to hormonal stimulation and egg pick-up, and they proposed some ways to make these experiences more bearable.
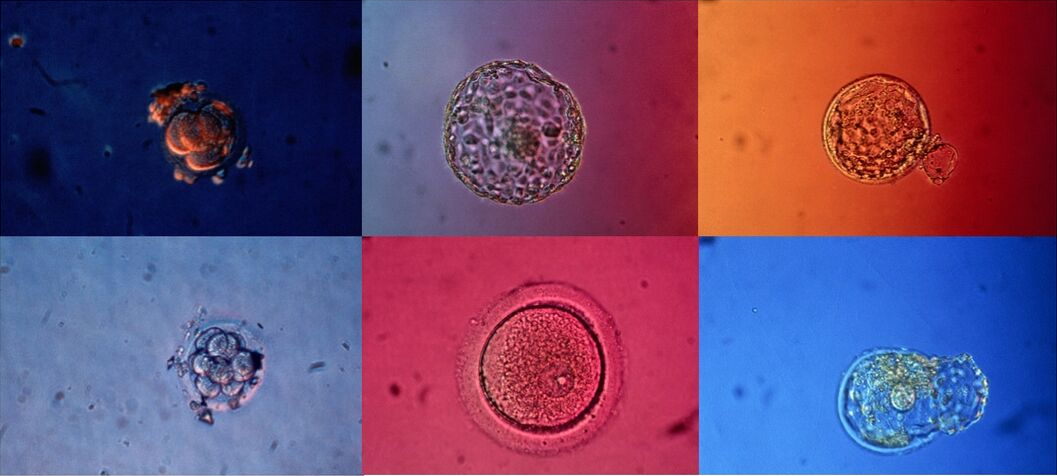
We had an interesting exchange about videos and images of embryos and how these may be received in very different ways according to when, where and how these were shared as well as personal preferences. We especially appreciated how people acknowledged each others’ points of view and how eager everyone was to hear about how research findings can contribute to improving care for patients.
These two workshops were the last of our 2021 public event series. We would like to sincerely thank everyone who has joined us for our events this year. Keep checking back on our Events page for information about our plans for 2022!
Over the past few months, the research team has participated in a number of events where we have discussed our findings and engaged in stimulating conversations with IVF patients and professionals (you can see a list of our past events and links to event reports on the Events page). In many of these conversations, we offered reflections based on the results of our social science research project, often focused on the debate on evidence and treatment add-ons. As this debate is very polarised, we have sought to highlight how our findings show a variety of perspectives on add-ons and their use, from the points of view of both professionals and patients. For instance, in our written evidence to the UK government’s Women’s Health Strategy, we underlined how the patients we interviewed expressed concerns regarding the abundance of information available online on IVF treatments (and especially add-ons) from multiple sources. Patients are exposed to a variety of claims without being able to assess their reliability. In contrast, the HFEA website offers impartial, accurate and up-to-date information, but this is currently limited to the evidence available to determine whether, for most fertility patients, a certain add-on is effective at improving the chances of having a baby.
Image 1: Visual representation of the HFEA’s traffic light system as of 9 November 2021.
This tool offers great clarity in terms of available evidence for both professionals and patients, but, as the evidence supporting add-ons is still scarce or of low quality, none of the add-ons on the list are currently green. In addition, and in some circumstances, add-ons may be offered for reasons other than to improve the chances of having a baby. To enable patients to better-understand the risks and potential benefits for each add-on, in April 2021 the HFEA included a list of questions that patients might ask their clinicians when discussing add-ons. These questions include a variety of aspects, such as: Is there good-quality evidence to back this up? Are there any associated risks or side effects from having this add-on? Am I assured that it is safe? and Do I know about any possible risks?
Both in our discussions with patients during our The IVF Experience events (which you can read about here and here) and in our interview with BBC reporter Sophie Sulehria as part of the Fertility Show’s live seminar series, we discussed these same issues, and how our research findings can support patients’ informed decisions. In particular, in our interviews with IVF professionals, different understandings of the meaning of the HFEA traffic light system emerged. Some interviewees understood the add-ons marked red as the problematic one, while they were more lenient toward those marked amber as they considered these promising. Other professionals, instead, were more worried about the add-ons marked amber. For this group in fact, add-ons marked red are clearly-identifiable as lacking supporting evidence, while amber ones might give patients the illusion of being more effective, while in actuality there is, equally, no evidence supporting them. Similarly, our interviews with patients show very different understandings of what constitutes “evidence”. Josie Hamper and I are currently working on an academic journal article that discusses four different approaches to evidence in relation to IVF treatment add-ons. While the majority of our patient participants preferred to delegate evaluations of evidence in IVF and follow the advice of their clinic or consultant in relation to treatment decision-making, other interviewees had a more direct assessment of evidence: some engaged in critical evaluations of evidence; others acknowledged the complex process of making evidence; and others relied on embodied experiences of evidence. With such a variety of points of views, a discussion on what kind of misunderstandings these may create with health professionals and institutional bodies is needed. We attempted to foster this discussion with one of our video animations: What is Evidence in IVF?
Drawing on our research and these discussions, we elaborated a proposal that goes in the direction of offering more information to patients, that we presented in our last workshop in collaboration with PET. In line with the ongoing HFEA discussion on how best to evolve the rating system for add-ons information and to consider the strength of the evidence base for each add-on, we suggested two main additions.
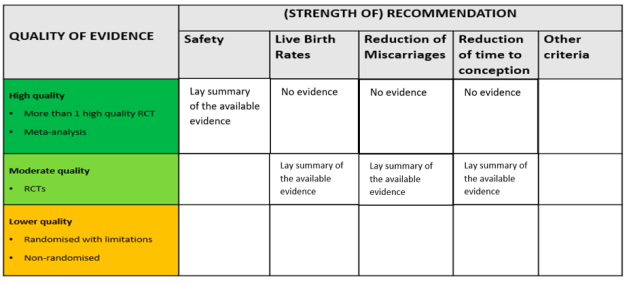
Image 2: Proposal for an infographic that offers further information for IVF patients about the evidence base for add-ons.
Firstly, we suggest including other criteria of evaluation for each add-on, including not only the available evidence on the ability of an add-on to improve the chances of having a baby, but also other relevant aspects for patients. This might include their safety and other potential effects on patients’ experience of IVF; for instance, the reduction of miscarriages and the reduction of time to conception. This would offer concrete support to make informed decisions for all the patients who are considering including add-ons in their treatment for reasons other than, exclusively, so as to improve the chances of having a baby. In addition, this would offer all patients more detailed information on each add-on, which they can then further discuss with their consultant.
Secondly, we suggest including additional indications on the quality of evidence available. Considering the current lack of quality evidence (i.e., more than one high quality RCT), including information regarding lower quality evidence – while highlighting that this evidence is not the best possibly available – would benefit those patients who need more clarity on why some recommendations are offered. In this case too, having reliable and detailed information available would enable patients to engage in conversations with their clinics on what the good-quality evidence they use to back up the use of add-ons is.
We anticipated two main disadvantages on offering such a detailed level of information: first, collecting and evaluating these different forms of evidence is time- and labour-intensive, and it would be a “village” effort requiring the collaboration of many members of the scientific community; second, making publicly available a summary of the currently available evidence would require agreement on a number of principles on what evidence should be included and what is too low-quality to be considered. Based on our findings, we believe being able to receive information from one reliable source would benefit many patients who are currently having to navigate information from a vast range of sources, many of which are less reliable.
During the workshop, an interesting discussion emerged on the use of the term “safety” among the criteria we suggested. For some workshop participants, this term is too ambiguous, means different things for various people and would be difficult to implement in terms of assessment. A suggestion by Katy Linderman, one of the guest speakers at the event, was to offer additional information on the potential “harm” that add-ons might have, including the risk of reducing the chances of having a baby through IVF. In line with the current HFEA discussion, it is extremely important to distinguish between the lack of evidence on a certain add-on, and the available evidence that an add-on is not safe (i.e. might somehow harm patients or reduce rather than increase their chances of having a baby through IVF).
Based on our research results and expertise, it is important for us to clarify: our proposal to share publicly the available evidence to best support informed decisions focuses on the content of the information that should be shared, rather than on how this is communicated. For this reason, we are not suggesting changes in colours or to add symbols in the visual representation of a ranking systems. Other research groups working on the best ways visually to share information are better positioned than us to provide recommendation on this.
On November 9th we had the pleasure to host another stimulating workshop, organised in cooperation with the Progress Educational Trust. For this online workshop we invited health professionals, researchers and fertility patient advocates to discuss the topics of evidence production and fertility treatment add-ons. This workshop was the third in a series of workshops designed for professionals (see our reports of previous workshops with the Royal College of Nursing and Progress Educational Trust).
The goal of this most recent workshop was to share ideas about: what kind of evidence can be produced in this field and how; what information is and should be available to patients in relation to the various treatments on offer; and how patients understand the evidence to support the treatments available to them.
In the first part of the workshop, Manuela Perrotta presented significant findings from our research project. She focused on the polarised debate on treatment add-ons and evidence-based medicine, by illustrating the current state of evidence available on treatment add-ons and exploring some of the reasons for lack of quality evidence. On the basis of the project findings, Manuela invited all participants to reflect upon what alternative information might be available publicly to patients interested in those treatment.
Some of the topics evoked were explored further by Sarah Armstrong, who underlined the importance of studying patients’ evaluations of complementary and add-on treatments in IVF. In the next presentation, Jack Wilkinson called into question the very definition of add-ons and resonated on how evidence is to be produced and communicated, not only in relation to whether or not specific treatments or equipment positively affect live birth rates, but also in relation to concerns about reducing chances of conception and live births.
Drawing on research data from IVF patient interviews, Josie Hamper took the (virtual) stage to introduce the different ways in which patients understand the concept of evidence in relation to their own IVF treatment journeys. Josie called for careful consideration of how patients’ personal evaluations of evidence shape their decision-making about add-ons. Josie’s talk was followed by Katy Lindermann, who stressed how, in a context of uncertainty about evidence in relation to complementary treatments and add-ons in IVF, some patients are interested in knowing whether these can produce any harm. She called for more research and information to be made public on the possibility of harm.
Among the most fruitful moments of this two-hour long workshop were the conversations that happened in breakout rooms, where all participants got the chance to express their positions, ask each other questions and react to the presentations. The option of offering patients additional information on every treatment on the HFEA website was considered a necessity, while participants discussed the pros and cons of the HFEA’s current traffic light system. Some acknowledged the challenges for health professionals in managing patients’ expectations and appreciated the need to continue having conversations with patients about the current state of add-ons.
Altogether, participants recognised the need to bring more people into these discussions, including some more of those who promote the use of add-ons. Participants broadly agreed that this would enable a more nuanced conversation about the quality of information that patients receive in order to make decisions about their own fertility journey.
This workshop was part of our public engagement event series. It was funded by a Wellcome Trust public engagement grant.
On 11 November we were happy to host the second workshop in our series The IVF Experience (see our report of the opening event here). Sarah Norcross from the Progress Educational Trust was our special guest for the second time and she succeeded in making our workshop such a welcoming and warm one. Everyone who joined us got the chance to respond to the research data that we presented, and many shared personal reflections from their own experiences. Some people spoke about what they considered to be especially important during their fertility journeys, others shared feelings or thoughts about the experience of being given embryo videos or images during their treatment.
Participants appreciated the opportunity to see how their own experience related to research data and findings and to the accounts of other participants, and some underlined how they got the chance to bring home feelings they had but hadn’t been put into words yet. It was so rewarding for us to see how our research could contribute to making some people feel more equipped to think back on their experiences, and how this event also allowed one of our participants to learn more about infertility and fertility treatment through exchanges with others.
We look forward to meeting more people at our next online workshops. Natalie Silverman will be with us on the 20th and 24th of November!
See our Events page for more details about how to sign up for the next dates.
The project team were present at this year’s Modern Family Show and the Fertility Show Online Summit. The timing of these shows presented a perfect opportunity for us to share our new animations, which you can watch on our website here.
Our booth at the Fertility Show Online Summit contained lots of details about the research project, our publications and, of course, our videos. The research team enjoyed visiting other booths as well as the many excellent seminars that were on offer across the four days. It was great to virtually ‘meet’ other show participants in the summit’s online chat.
Later in September, Manuela and I were interviewed by BBC reporter Sophie Sulehria as part of the Fertility Show’s live seminar series, which extended into the weeks following the online summit. We thoroughly enjoyed speaking to Sophie and having a conversation about fertility patients’ and professionals’ perspectives on IVF treatment add-ons.
We also screened our videos at the Modern Family Show, which took place in central London on 18 September. Unfortunately, the research team was unable to attend the show in-person, but the videos were screened on the main stage during the event for all attendees to watch.
We were thrilled to launch our online event series ‘The IVF Experience’ this week. Our first workshop coincided with Fertility Network UK’s National Fertility Awareness Week, which is an whole week dedicated to having conversations about infertility and the realities of fertility treatment.
Our first workshop was hosted by Sarah Norcross from the The Progress Educational Trust. Workshop participants had wide-ranging experiences of and relationships to IVF, which fostered really important conversations about the complexities of treatment decision-making for patients, feelings of control and lack of control, and the role of embryo images.
We are excited to have more conversations with others at our next workshops! See our Events page for information about how to sign up.
In June 2021, Manuela Perrotta and I submitted written evidence to the UK government’s Women’s Health Strategy for England. We believe the consultation presents a key opportunity to improve the treatment experiences of IVF patients.
In our response, which you can find in full on our Publications page, we make five policy recommendations:
Women need a more coordinated provision of up-to-date information about IVF, especially information about novel IVF treatment add-ons
Improving the clarity, visibility and accessibility of already available information is a relatively low-cost measure that will bring timely positive change for IVF patients
There is an opportunity for the NHS A-Z website to direct IVF patients to the Human Fertilisation and Embryology Authority’s website for information specifically about new IVF treatment add-ons
Different understandings of evidence should be considered to improve the quality of information on new treatment add-ons
Accurate information about the nature of available evidence should be provided when treatment add-ons are experimental
We are very grateful to Inflect Partners for their advice in preparing our submission for this call.
At the beginning of May we were delighted to spend an afternoon on Zoom with visual artist Sally Butcher, who is currently working on her Arts Council England funded project re.conceive. Sally approached us a while back to explore some of the synergies between our projects, which in different ways explore how reproduction, fertility and (non-)reproductive bodies are visualised or, sometimes, become invisible. Sally very generously shared some of her work-in-progress with us and we shared details about our research process and findings.
Each member of the research team was able to spend some time with Sally individually, and I include our reflections in our own words below.
Giulia: Sally’s work has inspired our conversation around reproduction in its different forms. We have especially discussed the relationship between medical knowledge, technologies and tools to visualise reproductive body parts or phenomena, and embodied experiences of them. We talked about the role of visual experiences in the construction of dominant narratives of gendered reproductive lives, and about the visibility and invisibility of specific reproductive experiences (for example infertility, miscarriages, abortion). We explored the notions of common and uncommon, known and unknown, expected and unexpected, we discussed how individual experiences relate to standardised measures and protocols and how people adjust and react to these, especially when these intersect with other medical, legal and geographical infrastructures (for example in the context of transnational reproductive travels).
Sally Butcher, Infertile Platitudes of Embodied Emptiness, Sonogram 7/9, Archival Inkjet Digitised Monoprint (2020). Used here with permission from the artist.
Manuela: Among the many things we talked about, Sally and I had an interesting conversation regarding some of her work-in-progress – in my interpretation, an inspiring visualisation of the current developments in the field of embryology. Sally’s representation of sets of data embedded within an image of an embryo captured the current turn in embryology, by highlighting visually the novel and increasing use of data-driven algorithms in this field. In our research, analysing the case of Time-lapse incubators and their incorporated algorithms, we have investigated how new knowledge about embryos is generated in the complex interactions between professionals and machines. Although the use of algorithms has the potential to release unknown biological information on embryos (and therefore reveal their hidden secrets), algorithms do not simply add medical and reproductive knowledge as they require human input and therefore still rely on professional expertise.
Sally Butcher, Human Algorithm V, pencil and pen on paper (2021). Used here with permission from the artist.
Josie: During our conversation, Sally and I found many shared interests: for instance in how themes of absence and presence, and proximity and distance, shape ideas about reproduction as well as experiences of infertility. Being a geographer (academically and at heart!), I was drawn to how the body exterior and interior are ‘mapped’ in some of Sally’s work. We talked about the role of measurements, ordering, boundaries and boundary-making in relation to how reproductive processes are visualised and described. We also talked about the intrigue and mystery of magnifying or looking inside things.
Sally’s work also drew my attention to all the other kinds of imagery that fertility patients encounter before or during their IVF treatment. The focus of our research is on images and videos of embryos, which are exterior to the body or in vitro. But fertility patients often encounter a whole range of other visualising techniques that allow them to see inside their bodies. Ultrasound scans and dye tests, for instance, are routinely used to medically investigate female reproductive organs and check that these appear to be functioning ‘normally’. Ways of visualising bodies and embryos have (personal and political) implications for how infertility is seen and known, and therefore very real consequences for patients’ treatment experiences and trajectories.
Sally Butcher, Sub-Maternal Exhaustion During a Pandemic, Archival Photograph, egg, ink and hand gel (2020). Used here with permission from the artist.
Sally: My conversations with the Remaking the Human Body team have been invaluable in my research project. As a visual artist, Re.conceive was driven by the invisibility of Infertility within the new wave of maternal visual arts, where, as in society at large, infertility still remains mostly hidden and shrouded in silence. My project aims to explore and visually theorise the transformational process of ‘becoming’ a (M)Other, challenging traditional reproduction to reconceive a form of sub-maternal.
My meetings with Giulia, Josie and Manuela helped thoroughly contextualise my thinking, aiding my understanding of how infertility connects with the broader narrative of reproduction, as well as giving me greater insight into the scientific procedures within embryology and new practices with AI, and drew my focus onto patient interpretation of these new technologies. It especially moved my thinking toward the visual and verbal languages used within infertility. As a cultural researcher, I am drawn to the rhetoric of medical terminology, weighted in ‘success’ and ‘failure’, aimed at potential ‘geriatric mothers’ with ‘inhospitable uteruses’, and how this may sit alongside hidden personal testimonies, confessional spaces of the coded #TTC online community, or conversations with family and friends where it so often generates a real sense of unease. As an artist, I try to use a feminist gaze to challenge institutionalised power within visual tropes of medical and commercial imagery of infertility. These meetings enlightened me as to how much power we place in these visuals and how these become naturalised into our knowledges of reproduction, with narratives of the embryo constructed from the encounters we have with these visuals. The immediate resonances I felt between my own practice and the fantastic work being done by this team, has encouraged me to continue using this imagery, exploring its symbolism alongside the power of the maternal imagination.