As part of our public engagement programme, we had the pleasure to host an extremely fascinating event ‘Time-lapse Imaging and the Debate on Evidence: A Social Science Perspective’, which we organised with the Progress Educational Trust (PET). For this event, we invited professionals involved in various aspects of IVF treatment to discuss, in a joint open conversation, some findings from our research regarding evidence production in IVF and patients’ perspectives on time-lapse embryo imaging.
In a two-and-a-half hour virtual meeting, Sarah Norcross, Jen Willows and Sandy Starr from PET moderated discussions in three break-out groups composed of gynaecologists, embryologists, nurses and counsellors who specialise in fertility. Project lead, Manuela, and researcher, Josie, introduced the project and its main results concerning the production of evidence in relation to time-lapse embryo imaging tools, and patients’ experiences of receiving videos of embryo development produced by these tools.
First, the three groups discussed the role of evidence in relation to IVF treatment and time-lapse embryo imaging in particular. Questions were raised about how evidence should be produced in the field of IVF, what counts as evidence and how different kinds of evidence production may be taken into account when making decisions about offering certain tools or treatments. Some conversation happened around how different perspectives come into play when considering time-lapse embryo imaging devices as lab equipment rather than as a part of treatment. Some of the discussions encouraged us to pay attention to the benefits for each actor involved when a new tool is being used in the lab. A few participants were especially interested in the underlying economic implications of considering time-lapse embryo imaging as an add-on to fertility treatment or, on the contrary, an investment for the lab. Some underlined how these two are embedded elements of IVF services when it comes to the private sector.
Manuela and Josie also called the audience’s attention to the need for fertility professionals to reflect upon how time-lapse embryo videos are shared with patients, where this happens, and when in relation to patients’ treatment and medical encounters. Workshop participants were confronted with quotes and questions about patients’ relationships to embryo images and videos during and after IVF treatment and they were asked to reflect upon their own professional experience with this. Counsellors especially shared experiences about patients who had particular relationships to visuals during treatment and underlined how communication around such imagery is key to patients’ understanding of their treatment.
At the end of the workshop, some of the participants expressed their intention to build reflections that emerged from the workshop into their work practice, especially about how and when to share images and videos with patients, and how to make this a positive experience for them.
Three months after our event on Visions of Reproduction at the Being Human Festival, we are glad to offer a new way to engage with our research project. If you are more comfortable with hearing than reading about vision (no jokes!), connect and listen to the wonderful podcast that Natalie Silverman has produced for The Fertility Podcast (also embedded below).
In this podcast, Natalie accompanies the audience through the topic of visualising reproduction in historical, sociological and aesthetic terms, introducing and interrogating expert scholars and artists whose work dives into visual representations of conception, pregnancy, and miscarriage. The listening experience is a gripping one, where vision becomes imagination, shaped by the words of people who describe the making and meaning of imagery in ancient books, biology labs, contemporary fertility clinics, and in personal artistic creations and performance. We hope you enjoy!
I had the pleasure of attending this year’s online Progress Educational Trust (PET) annual conference where the topics for consideration were fertility, genomics and COVID-19.
Consultant Jane Stewart opened the first session by speaking about the experiences of fertility clinics and she used the surfing analogy of ‘riding the wave’ through what was, and still is in many respects, a great unknown. One of the difficult issues for clinics throughout has been how to organise their reopening and patients’ return to treatment, where a more restricted allocation of resources can necessitate the prioritisation of some patients over others. This issue was taken up by philosopher and bioethicist Julian Savulescu, who described IVF as a ‘playground of ethical issues’. For instance, considerations about what constitutes elective treatment, non-urgent treatment, futile treatment, risk and safety involve a series of value judgements that are contestable. The ways in which fertility clinics approach the pandemic and its aftermath will likely involve judgements about how to prioritise the return of fertility patients, and Julian set out various ways to go about this process of prioritisation:
Should fertility treatment be offered on a first-come first-served basis? Should older patients receive treatment first given that they might be under greatest time pressure? Or should patients who have highest chance of success be given first access?
There are no clear or straightforward answers to which of these options is right or fair, but it is clear that decisions made at the clinic level will have a deep impact on patients’ lives. The uncertainties involved for patients about their treatment progression during the pandemic was taken up again in Session Four by chair Anna Veiga, who noted that there has been an increase in people seeking elective egg-freezing services during the pandemic as they anticipate a treatment delay of an unknown length of time.
Sessions Two and Three emphasised the wide range of unknowns about how COVID-19 – or more specifically the virus SARS-Cov-2 – affects reproductive function, semen, oocytes and foetuses. Allan Pacey, professor of andrology, noted the vast amount of research that has been done on this topic but he also emphasised the importance of maintaining quality assurance in all research. Session chair Fiona Fox reiterated the need to be cognisant and critical of a current infodemic, where poor research is given a platform and circulated in rapid media reporting. While the findings from studies on reproduction and SARS-Cov-2 so far are often inconclusive or difficult to extrapolate to the population level, the panels were largely positive about the low risks of the virus during fertility treatment and pregnancy, as well as for longer term fertility, yet they also insisted that this does not take away the fact that for some individuals COVID-19 can have devastating effects. Geneticist Sharon Moalem offered some fascinating insights into why men seem to be more susceptible to COVID-19 than women. Reflecting differential responses to many other viruses, female immune systems show a greater antibody response to infection, which impacts on the body’s resilience to severe illness as well as its response to vaccination.
The fourth session focused on the guidelines for fertility clinic reopening that have been developed by the European Society of Human Reproduction and Embryology. In practice, experiences from clinics have involved putting into place new staff and patient testing procedures, as well as sanitisation measures and the offering of telemedicine. While there was a sense that clinics have been able to respond to the new requirements effectively, concerns were expressed throughout the conference about limitations in other essential medical and health services. Specialist in reproductive medicine Luca Gianaroli noted that stillbirth rates have increased in many European countries, including the UK, during the pandemic. This, he said, is not due to the virus itself but rather the reduced access to antenatal and emergency care services. The impacts of reduced healthcare access was echoed by Human Fertilisation and Embryology Authority (HFEA) chair Sally Cheshire earlier in the day, who described how patients at the early stages of seeking diagnostic examinations via their general practice or routine gynaecological surgery are at a disadvantage in their potential fertility treatment progression. While there was a sense that fertility clinics have been able to respond relatively well to a new way of working, many other areas of the health services in the UK are experiencing backlogs and increased waiting times. These cases emphasised how fertility treatment is not an isolated ‘moment’ or procedure, but that it is closely tied to reproductive health more broadly as well as antenatal health and care. Attending to fertility patients’ broader trajectories of treatment is central to gaining a fuller understanding of the impact of the pandemic in this area.
Natalie Silverman, founder and voice of the Fertility Podcast, led the audience through our first event ‘Visions of Reproduction’ where speakers shared and discussed a wide range of videos, pictures, drawings, prints and embroideries of embryos, foetuses, pregnancy tests, pregnant and not pregnant bodies.
As part of this event, we ran a poll among the audience asking them (anonymously) to enter three images about reproduction that they had come across in their life. We received so many fascinating responses! Pregnancy tests, ultrasound and embryo were definitely the most chosen words, but people had also come across paintings, celebrity pregnancy photos, a real-life foetus-museum, 3D scans and many more. People are confronted with reproductive images multiple times in their lives and in very different situations.
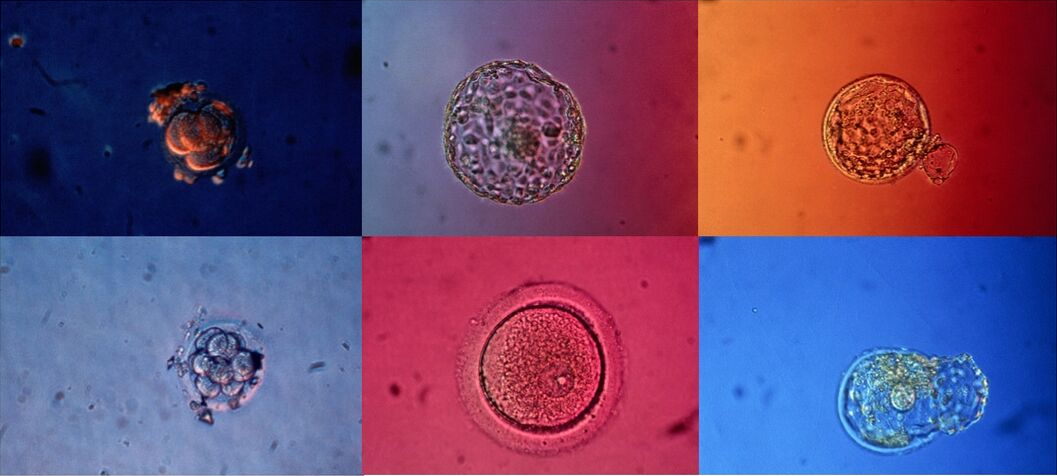
Josie Hamper, from our research team, opened the event by presenting some unpublished results from the study. She launched a poll where the audience was invited to select the correct description for an image shown on-screen. People selected almost all available answers, including: A human embryo; An IVF embryo; Eight cell embryo; Grade one embryo; A potential baby; and baby’s first picture. It was revealed that all answers did in fact describe the image and that the diverse responses reflect different perspectives according to people’s expertise, experience or agendas. Josie accompanied the audience through the data of her own research on IVF patient’s experiences of receiving time-lapse videos of embryo development. She illustrated how videos may be welcome by some who receive them, while creating more uncertainties for others, especially if they feel unequipped to interpret what they are seeing. She ended by inviting a more nuanced public discussion around time-lapse embryo imaging technology, and the use of the videos and images that derive from this technology, beyond the clinic.
This question was taken up by Tabitha Moses who talked about her artwork around IVF experiences, involving photography and intricately embroidered hospital gowns. She accompanied the audience through the experience of various visualising technologies throughout infertility journeys, IVF treatments and pregnancy loss, and she discussed the possibility of trusting or privileging the feeling of a pregnancy through quickening or other embodied sensations, including those of pregnancy loss, over the images produced through medical technologies.
Tabitha Moses, Investment, Tabitha, 2014. Photo portrait by Jon Barraclough. Used here with permission from the artist.
Isabel Davis developed the theme of vision versus feeling in her talk on the history of potential pregnancy. She dealt with the experience of un-pregnancy, meaning the condition of not really being pregnant yet but possibly being, through the work of natural scientist William Harvey on non-generation. Isabel’s talk prompted us to reflect upon ambiguous moments after a non-protected heterosexual intercourse takes place or after an embryo transfer where someone may wonder whether or not a pregnancy has started. These are all important dimensions of reproductive imagination and experience.
The topic of the uncertain time where pregnancy is not (yet) but could be is something Liv Pennington also reflected on when she talked about her artwork on pregnancy tests and the challenges of photographing them on different occasions. Liv’s talk accompanied the audience through her performative artwork Private View, which took place in 2002 and in 2019, and how the performance differed in so many ways between these dates as people’s relationships to pregnancy tests, images and sharing have changed, for instance through the increased familiarity with sharing and commenting on images via social media. Liv reflected on how visualising a pregnancy test result opens up possibilities that may change over time and how this makes her work controversial because of the vulnerability involved in exposing someone’s private reproductive moment while acknowledging the dynamic and uncertain process of pregnancy.
Liv Pennington, Private View, 2006. Used here with permission from the artist.
Funnily enough, technical issues prevented Liv from sharing her slides with the audience, which meant that we relied on Liv’s descriptions of her images, her facial expressions and ability to represent pictures through words. An experience that turned out to be powerful for an event on visualisation!
Nick Hopwood was the last speaker on the panel. His contribution proposed a long-term historical perspective on images of embryos and foetuses to unpack how the ordering of these along a narrative of development has, since the late eighteen century, come to stand for the course of a pregnancy. Nick underlined how images of reproduction produced over the last centuries have overwhelmingly represented a linear process, leaving out experiences of miscarriage or unsuccessful stories of fertility treatment, both of which are frequent ‘events’ in people’s reproductive lives, but underrepresented and thus erroneously considered the exception.
A conversation among all the speakers, with questions asked by the audience, allowed everyone to engage with the common threads or connections among such different approaches to common and less common reproductive images. The conversations highlighted how these images evoke questions of temporality in reproductive processes; how selection and standardisation have been embedded in the use and fruition of images concerning reproduction in the last centuries; and how images have been used for defining normality, normal variations and abnormality. The talks and discussion especially emphasised how a certain production and use of images facilitates the diffusion of dominant narratives of reproduction, leaving out meaningful and relevant experiences, which do not find space in the public representation.
—
We are exceptionally grateful to all the speakers and the audience who made this panel so engaging and rich in content. We also want to extend our thanks to the Centre for Public Engagement at Queen Mary and the Being Human Festival for making this event possible.
Keep an eye out for further details about our next events!
We are very excited to introduce our first public engagement event after a series of cancellations earlier this year. This online event is entitled Visions of Reproduction: The Making and Meaning of Reproductive Imaging and it brings together sociologists, historians and artists who will speak about their work on this theme. We are also delighted to have partnered with the Fertility Podcast founder Natalie Silverman, who will moderate the event and take questions from the audience.
Join us on 12 November 2020 at 6pm.
For more information and a link to the booking site, please visit the Being Human Festival event page.
With the closure or limited opening of fertility clinics due to the pandemic, fertility patients have had much fewer opportunities to connect with professionals through open days or fertility fairs, which prompted the magazine IVF babble to organise a live online Fertility Expo. I attended the event on 19 July and was able to explore a virtual showroom with over 50 booths belonging to fertility clinics, charities and other specialists. Many of the booths were staffed via a live chat function and offered the option to book online consultations. In the ‘auditorium’ I attended live talks about evidence and add-on treatments, the connections between stress and fertility, and the role of a fertility coach, as well as a panel session on self-care while trying to conceive, and I watched two short films explaining how Embryoscope works. The range of topics explored was impressive.
I was particularly struck by the international spread of speakers and clinics represented at the expo. While it comes as no surprise that fertility treatment crosses borders, travel within and between countries has become synonymous with risk and danger during the pandemic. Restricted travel has had huge impacts on planned or initiated fertility treatment abroad and media reports have described desperate situations where people have been unable to retrieve babies from surrogates (see here). Inevitably these new risks and limits to mobility will place additional stress on a process that can already feel risky at every stage.
The idea of avoiding unnecessary risk has become a familiar frame of mind over the last couple of months, although for patients in the midst of fertility treatment, calculations of necessity and risk are highly complex, emotional and shifting. Back to the expo, many of the talks I attended seemed to assume that the world of fertility treatment will be returning to ‘normal’ at some point in the not-too-far future, yet I questioned to what extent this will be the case. I wondered what long-lasting impacts the pandemic will have on the landscape of fertility treatment, patients’ decision-making processes and their maintenance of hope, as these respond to a contemporary moment of uncertainty.
Update (31 March 2020): We have decided to also postpone our three May workshops. We plan to re-schedule all of our events for the autumn.
Update (14 March 2020): Following careful consideration of the current COVID-19 pandemic, we have decided to postpone our March workshops. We will evaluate whether our May events can go ahead in due course. Please check back for updates and we hope to see you on a future date!
We invite you to a workshop where all will have a chance to participate in a conversation about infertility, fertility treatment, scientific knowledge, embryo/medical imaging and patient decision-making. You will have the opportunity to hear more about our ongoing research in the area.
There will be snacks and drinks and lots of space for sharing ideas, opinions and experiences.
The workshop will take place in London on five dates across March and May 2020. For more information and to book your place, follow the links to our eventbrite pages:
CANCELLED 14 March 2020. Timber Lodge café, 1A, Timber Lodge Queen Elizabeth Olympic Park, Honour Lea Ave, London E20 1DY. Starts at 2.30pm. SIGN UP HERE.
CANCELLED 17 March 2020. The Vagina Museum, Unit 7&18 Stables Market, Chalk Farm Road, London, NW1 8AH. Starts at 6.30pm. SIGN UP HERE.
CANCELLED 13 May 2020. Yurt café, St. Katharine’s Precinct, 2 Butcher Row, London E14 8DS. Starts at 6.30pm. SIGN UP HERE.
CANCELLED 16 May 2020. Poplar Union, E5 Roasthouse, 2 Cotall St, Poplar, London E14 6TL. Starts at 2.30pm. SIGN UP HERE.
CANCELLED 28 May 2020. The Canvas: Café & Creative Venue, 42 Hanbury St, Spitalfields, London E1 5JL. Starts at 6.30pm. SIGN UP HERE.
These events are funded by the Wellcome Trust and supported by Fertility Network UK.
The Progress Educational Trust’s (PET) annual conference has become an established event in our December calendar and this year we continued the tradition. This year’s conference was entitled ‘Reality check: A realistic look at assisted reproduction’ and dealt with a range of topics including evidence, regulation, informed choice for patients and the ongoing ‘add-on debate’ (which I wrote about in a previous post). In total, there were 14 talks across the day, with each session followed by an opportunity for the audience to ask questions or offer comments to the speakers. In this post, I am going to reflect on some issues around evidence that emerged throughout the day.
We have entered ‘an era of profound unreliability’ said James Duffy in his talk about the production of evidence in which he detailed how research being done in the field of assisted reproduction often falls short of accepted standards of scientific rigour. For instance, findings from trials that are run entirely in one clinic cannot be translated to other clinics or patient populations, and he contended that research is often driven by commercial interests rather than an interest in the production of ‘gold standard’ evidence. Yet Nick Macklon explained how the reliance on randomised control trials (RCTs) in assisted reproduction research sets a very high bar for what counts as acceptable evidence, at the risk of ignoring other valuable data that are produced outside of the RCT framework. While RCTs are, with good reason, considered to offer the highest level of evidence in medicine, there are significant barriers to conducting RCTs in infertility research; challenges include the large required sample size, the long timeline from research design to implementation and results, and the issue of the trial sample not reflecting the patient group due to strict participant selection criteria. We were reminded that IVF was highly controversial and not supported by an RCT when developed in the 1970s (as I learnt from my visit to the Science Museum), which could serve as an argument both for tighter regulation and monitoring, as well as the benefit of allowing space for technological and scientific innovation. Sally Cheshire, chair of the Human Fertilisation and Embryology Authority (HFEA), brought the attention back to the patient in her speech (available in full here), emphasising that while it is crucial to continuously develop and improve IVF procedures we need to critically question whether it is fair for patients to pay for this knowledge production, especially if it could potentially cause physical, psychological or financial harm.
Another point that complicates the issue of evidence in contemporary fertility treatment is the discrepancy between what is offered in IVF clinics and the recommendations provided by the HFEA. Søren Ziebe opened the first session with a provocation whereby he questioned why over half of IVF cycles use pre-implantation genetic screening (PGS) when the HFEA determines this procedure to be without reliable evidence that it improves chances of pregnancy. Later in the day, Chris Barratt also argued that intracytoplasmic sperm injection (ICSI, where the sperm is injected directly into the egg) is vastly overused in fertility clinics. ICSI is used in over half of IVF cycles despite the HFEA and National Institute for Health and Care Excellence (NICE) guidelines stating that this procedure should only be used for male-factor infertility, which accounts for only about a third of infertility cases.
The fact that practices of fertility clinics go against national recommendations on such a large scale sends contradictory messages to patients, which can cause feelings of confusion and suspicion of professional judgement. These feelings are further amplified by the issue of significant gaps in current knowledge about reproductive biology and assisted reproduction; unexplained infertility and failed implantation emerged several times across the day as significant grey areas with an urgent need for better understanding. In the discussion sessions there was some conversation about the complexities of doctor-patient consultations as sites where the practice of evidence-based medicine intersects with individual clinical practice and patients’ needs, wants and choices. While debates about add-ons have been ongoing for years, it is on the ground, in the fertility clinic consultation room, that the actual discussions with patients about add-ons takes place. One practicing fertility specialist noted how, rather than simply running a search for evidence in a medical database and recommending fertility treatment based on this, consultations are more akin to a conversation and negotiation between the doctor and patient. Others noted how it can be extremely difficult to say ‘no’ to a patient who has a strong belief in or desire for a particular treatment or test regardless of its evidence-base, especially when the patient will potentially go elsewhere and pay for it. Explaining the mixed evidence for certain procedures is challenging in a situation where patients are often willing to take great chances in the hope that a treatment might work.
The vast exhibition hall of the London Fertility Show felt strangely familiar this year as I have come to recognise company stands, logos and people from previous years. A slight difference this year was the presence of a branch-out Fertility Fest, which is always of particular interest to me given the focus of my work on the patient experience of IVF.
My first session of the day was called ‘When Plan B was Meant to Be’ and opened with a reading by Lisa Faulkner from her recently published book ‘Meant to Be: My Journey to Motherhood’. The reading set the scene for an open discussion about the emotional toll that fertility treatment takes on people, the difficult decision of when and how to stop trying, and what happens after IVF that did not result in a baby. Faulkner honestly articulated the enduring grief that follows ‘failed’ IVF while also conveying how a life without adoption, which was originally her Plan B for motherhood, is now unimaginable. Faulkner was joined on stage by fertility specialist Mohamed Taranissi, who offered his perspective on the importance of a personalised treatment procedure that attends to emotional wellbeing. Together they made a case for the importance of close communication between patient and doctor.
From there I attended ‘The Invisible Man’, which dealt with the male experience of infertility. Rod Silvers took to the stage with a personal provocation to the audience that set out a series of traditional male values that impact on men’s experiences of infertility. Silvers emphasised the intimately felt desire and expectation to ‘be the strong one’ in his relationship. Joined by Russell Davies, a fertility coach, and Sheryl Homa, a clinical scientist with a particular interest in male fertility, they challenged the widely accepted fact that women’s bodies are the prime focus of fertility tests and treatments, emphasising that there needs to be a more proactive testing of male fertility as routine in general practice healthcare. They also reflected on the absence of men’s voices in conversations about the emotional impacts of fertility treatment: they emphasised the importance of men talking to other men and lamented the decline of what Davies called ‘men talking around the campfire’ as a form of male peer support.
Entangled throughout discussions of the emotional aspects of infertility, control repeatedly emerged as an important theme: being in control and letting go. Faulkner described the huge relief of handing over control to her fertility specialist and how this gave her the feeling of ‘being carried’ through IVF. Silvers and Davies also spoke about the expectation that men should be the ones to ‘hold it together’ and guard their emotions. There are no established cultural tropes for men’s struggle with the emotional strain of IVF, which plays a part in the absence of men’s voices in discourses of infertility. I wondered about the phrase ‘holding it together’ and thought that the image of holding something – like loss and grief – together seemed pertinent to these discussions about the importance of talking to, caring for and supporting each other.
The designated Fertility Fest room seemed to offer an important space for attendees at this year’s show to hear real voices, conversations and personal experiences. This was a space where people could express their sadness – the sessions both opened with a Fertility Fest trailer where co-founder Jessica Hepburn states that ‘crying is good, isn’t it’. But it was also a space for joking and laughter. This acknowledgement of conflicting emotions reminds us, I think, of what the creative arts are particularly excellent at doing, which is bringing together tragedy and comedy in a way that is sensitive and honest to the complexities of personal experiences of coping, getting by and moving on.
The RHB team had a productive summer with amazing conferences and manuscript writing. Having received so much useful feedback as of late, we are ready to publish some of the first project findings. The conferences we attended in the past months have really helped us contextualize our research and hone our arguments.
In August, RHB was at the annual meeting of the American Sociological Association, where we were part of one of the five (!) Sociology of Reproduction panels. Given that RHB is UK-based, we were able to assess how the issues raised in our research relate to wider concerns regarding technology, medicine, and reproduction. Although the UK IVF conversation has lately involved a sustained critique of commercialisation, audiences have remarked that the industry here is quite tightly regulated when compared to other countries (the U.S. especially), where healthcare is largely driven by a strong consumer logic. This is particularly true of fertility treatment, where multiple IVF cycles can cost tens of thousands of US dollars. As reproduction researchers, however, we strongly feel that fertility care should be an integral part of public healthcare services for all.
The ethics of new biomedical technologies was the focus of the first of our two panels at the 4S (Society for Social Studies of Science) meeting in late summer. Here, scholars raised excellent questions about the introduction of new medical technologies and the value they add to practice. As we have grappled with the role of time-lapse in IVF, we have found that the meanings of this technology can be different depending on one’s position and perspective. For example, time-lapse can be a great lab tool for embryologists, while also a reassuring technology for patients who want to know that their embryos are kept in a stable environment 24/7. This is an aspect of time-lapse that our audience has found incredibly interesting.
We have also recognized in our presentations that efficiency evidence is currently an important criteria for assessing new IVF technologies, especially in the UK add-on conversation. Based on our findings so far, this is one of the most salient themes that arises when talking to professionals about the value of new treatments. In the near future, we aim to publish our data on how fertility professionals in the NHS conceptualise evidence and its relation to time-lapse tools. In the meantime, we are also working on finishing up data collection, so that we can share findings on patient perspectives as well in the coming year. Last but not least, planning for public engagement activities in underway, with several events that will take place in 2020. Stay tuned!