At the beginning of May we were delighted to spend an afternoon on Zoom with visual artist Sally Butcher, who is currently working on her Arts Council England funded project re.conceive. Sally approached us a while back to explore some of the synergies between our projects, which in different ways explore how reproduction, fertility and (non-)reproductive bodies are visualised or, sometimes, become invisible. Sally very generously shared some of her work-in-progress with us and we shared details about our research process and findings.
Each member of the research team was able to spend some time with Sally individually, and I include our reflections in our own words below.
Giulia: Sally’s work has inspired our conversation around reproduction in its different forms. We have especially discussed the relationship between medical knowledge, technologies and tools to visualise reproductive body parts or phenomena, and embodied experiences of them. We talked about the role of visual experiences in the construction of dominant narratives of gendered reproductive lives, and about the visibility and invisibility of specific reproductive experiences (for example infertility, miscarriages, abortion). We explored the notions of common and uncommon, known and unknown, expected and unexpected, we discussed how individual experiences relate to standardised measures and protocols and how people adjust and react to these, especially when these intersect with other medical, legal and geographical infrastructures (for example in the context of transnational reproductive travels).

Sally Butcher, Infertile Platitudes of Embodied Emptiness, Sonogram 7/9, Archival Inkjet Digitised Monoprint (2020). Used here with permission from the artist.
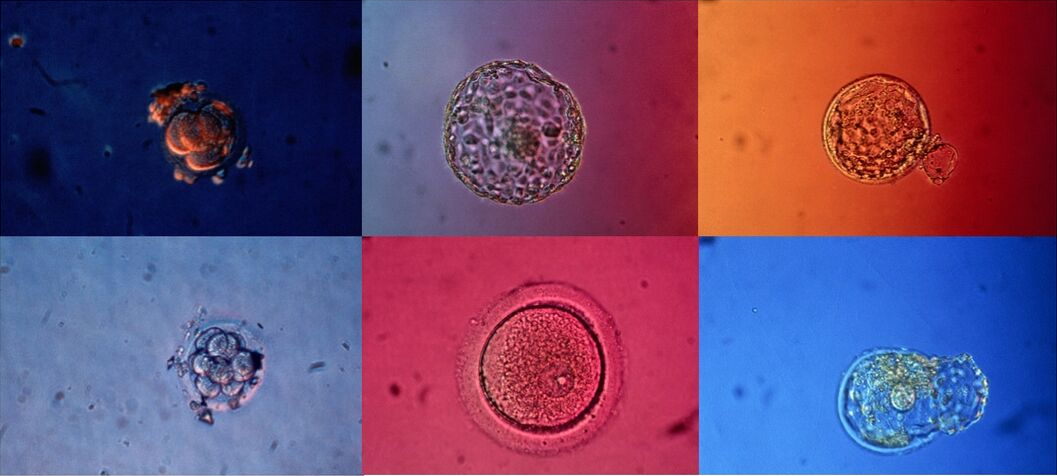
Manuela: Among the many things we talked about, Sally and I had an interesting conversation regarding some of her work-in-progress – in my interpretation, an inspiring visualisation of the current developments in the field of embryology. Sally’s representation of sets of data embedded within an image of an embryo captured the current turn in embryology, by highlighting visually the novel and increasing use of data-driven algorithms in this field. In our research, analysing the case of Time-lapse incubators and their incorporated algorithms, we have investigated how new knowledge about embryos is generated in the complex interactions between professionals and machines. Although the use of algorithms has the potential to release unknown biological information on embryos (and therefore reveal their hidden secrets), algorithms do not simply add medical and reproductive knowledge as they require human input and therefore still rely on professional expertise.

Sally Butcher, Human Algorithm V, pencil and pen on paper (2021). Used here with permission from the artist.
Josie: During our conversation, Sally and I found many shared interests: for instance in how themes of absence and presence, and proximity and distance, shape ideas about reproduction as well as experiences of infertility. Being a geographer (academically and at heart!), I was drawn to how the body exterior and interior are ‘mapped’ in some of Sally’s work. We talked about the role of measurements, ordering, boundaries and boundary-making in relation to how reproductive processes are visualised and described. We also talked about the intrigue and mystery of magnifying or looking inside things.
Sally’s work also drew my attention to all the other kinds of imagery that fertility patients encounter before or during their IVF treatment. The focus of our research is on images and videos of embryos, which are exterior to the body or in vitro. But fertility patients often encounter a whole range of other visualising techniques that allow them to see inside their bodies. Ultrasound scans and dye tests, for instance, are routinely used to medically investigate female reproductive organs and check that these appear to be functioning ‘normally’. Ways of visualising bodies and embryos have (personal and political) implications for how infertility is seen and known, and therefore very real consequences for patients’ treatment experiences and trajectories.

Sally: My conversations with the Remaking the Human Body team have been invaluable in my research project. As a visual artist, Re.conceive was driven by the invisibility of Infertility within the new wave of maternal visual arts, where, as in society at large, infertility still remains mostly hidden and shrouded in silence. My project aims to explore and visually theorise the transformational process of ‘becoming’ a (M)Other, challenging traditional reproduction to reconceive a form of sub-maternal.
My meetings with Giulia, Josie and Manuela helped thoroughly contextualise my thinking, aiding my understanding of how infertility connects with the broader narrative of reproduction, as well as giving me greater insight into the scientific procedures within embryology and new practices with AI, and drew my focus onto patient interpretation of these new technologies. It especially moved my thinking toward the visual and verbal languages used within infertility. As a cultural researcher, I am drawn to the rhetoric of medical terminology, weighted in ‘success’ and ‘failure’, aimed at potential ‘geriatric mothers’ with ‘inhospitable uteruses’, and how this may sit alongside hidden personal testimonies, confessional spaces of the coded #TTC online community, or conversations with family and friends where it so often generates a real sense of unease. As an artist, I try to use a feminist gaze to challenge institutionalised power within visual tropes of medical and commercial imagery of infertility. These meetings enlightened me as to how much power we place in these visuals and how these become naturalised into our knowledges of reproduction, with narratives of the embryo constructed from the encounters we have with these visuals. The immediate resonances I felt between my own practice and the fantastic work being done by this team, has encouraged me to continue using this imagery, exploring its symbolism alongside the power of the maternal imagination.

